


Written by Dr. Diane Mueller
ELISA test for Lyme disease is often the first blood test a doctor orders when Lyme is on the table. But this is where many patients get tripped up: a screening test is not the same thing as a final answer.
I’ve seen this pattern again and again in patients who come to us after months or years of being told they’re fine because one test was negative. If you live in a place like Austin, Texas, where people spend time on trails, greenbelts, and wooded edges around neighborhoods like Barton Creek, tick exposure is not some distant theory. And if you have fatigue, joint pain, brain fog, headaches, or strange nerve symptoms, you need to know what the ELISA can do, what it can miss, and what to do next.
If you’re wondering ‘which is the best test?’, head on over to our Best Lyme Disease Test guide.
The ELISA test for Lyme disease is a first-line screening tool that checks for antibodies, so it cannot confirm or rule out Lyme disease by itself.
Timing matters because the ELISA test for Lyme disease may be negative in the first 2 to 6 weeks before your body makes enough antibodies to detect.
A positive ELISA usually needs confirmatory testing, while a negative result should still be weighed against symptoms, rash history, and likely tick exposure.
False negatives and false positives can happen, especially in early infection or when other immune activity affects the test response.
If Lyme symptoms fit but your ELISA is negative, document your timeline, ask about repeat testing in 2 to 4 weeks, and request a full clinical evaluation.
A stronger Lyme assessment combines lab results with exposure history, multi-system symptoms, and clinical judgment instead of relying on one screening result.
The ELISA test for Lyme disease measures your immune system’s response to Borrelia burgdorferi, the main bacteria linked to Lyme disease in the US. It does not usually look for the bacteria directly. It looks for antibodies, most often IgM and IgG, that your body may produce after exposure.
That one detail changes everything. If your immune system has not made enough antibodies yet, the test can be negative even when symptoms are real.
The ELISA is an enzyme immunoassay, also called an EIA. In simple terms, a lab places Lyme-related antigens on a testing surface. If your blood contains antibodies that recognize those antigens, they bind. Then the lab adds an enzyme-linked marker that creates a color change. More signal usually means more antibody activity.
Common antigens include C6 peptide, OspC, and flagellin. Some newer versions, especially C6 ELISA, tend to perform better than older whole-cell tests.
Research summarized in clinical reviews shows that C6-based testing can have specificity around 97% to 99%, while sensitivity improves as infection progresses.
Action step: Ask which ELISA version your lab used and whether it included C6. That takes 2 minutes and gives you better context for the result.
ELISA is often the first test because it is fast, lower cost, and useful for screening large numbers of samples. Public health systems and standard medical practices use it as step one in a two-tier testing algorithm.
Here is the basic flow:
Step 1: Run an ELISA or EIA screening test
Step 2: If positive or sometimes equivocal, run confirmatory testing
Step 3: Interpret the result with symptoms and exposure history
This approach works well in many straightforward cases. It is also practical for clinics in busy regions like Central Texas, where physicians need a standard process.
But first-line does not mean perfect-line. It means screen first, confirm next. For patients with complicated illness, that distinction matters a lot. The ELISA test is just one piece of the puzzle, getting an accurate Lyme disease diagnosis often requires a combination of clinical evaluation and follow-up testing.
Action step: If your doctor says, “Your ELISA was negative, so it’s not Lyme,” ask whether they are following a full clinical evaluation or stopping at the screening stage.
We have helped thousands of people in Colorado, Wyoming, New Jersey, Pennsylvania, Texas, Wisconsin restore their health and quality of life by diagnosing and treating their Lyme Disease.
The accuracy of the ELISA test for Lyme disease depends heavily on timing, test design, and the stage of illness. That is the short answer. The longer answer is why so many people get confused.
In early Lyme, sensitivity can be poor, with reports ranging from about 17% to 74%, and even 29% to 48% in early localized infection. In later disease, sensitivity may rise sharply and can approach near 100% in some studies. Specificity improves further when ELISA is followed by confirmatory testing.
For a practical overview of how different options compare, see this article on best Lyme disease test.
A false negative happens when the test says no Lyme antibodies are present, but the person may still have Lyme. A false positive happens when the test reacts for another reason.
False negatives can happen when:
The infection is still early
Antibodies have not risen yet
The immune response is uneven
The test panel does not catch the relevant antibody pattern
False positives can happen because of cross-reactivity. Other infections or immune activity can sometimes trigger a signal. Older test formats had more of this problem. Past OspA vaccination also affected some earlier testing approaches.
This is why ELISA should not be treated like a stand-alone verdict in a patient with a complicated story.
Action step: If your result does not fit your symptoms, request the exact lab name, test type, and index value. Keep a copy for your records.
Timing is one of the biggest reasons the ELISA test lyme disease result can mislead people. Your body usually needs 2 to 6 weeks to build a measurable antibody response.
That means a person can be bitten by a tick, feel awful 10 days later, get tested, and come back negative. I’ve seen that exact scenario. The patient feels feverish, achy, foggy, and scared. The lab says “negative,” and the case gets dismissed too fast.
This problem matters even more if you had a bull’s-eye rash, summer flu-like symptoms, or a clear outdoor exposure near parks, trails, or brushy lots around Austin. A negative early ELISA does not erase that history.
For a broader look at timing and interpretation, this article on how Lyme is diagnosed and why it gets missed is useful.
Action step: If exposure was recent, ask whether you should retest in 2 to 4 weeks. Put that date on your calendar today.
A positive ELISA test for Lyme disease suggests possible exposure, not automatic proof of active Lyme disease. A negative ELISA lowers suspicion in some cases, but it does not always rule Lyme out.
That sounds less clean than most people want. But it is the honest answer.
In standard CDC-style two-tier testing, a positive or equivocal ELISA usually needs a confirmatory test, historically a Western blot and, in some settings, a modified two-tier algorithm using another immunoassay.
Why? Because screening tests are built to catch possibilities. Confirmatory tests help narrow down whether that signal is more likely to be real.
Some data suggest that a high ELISA index value, such as 3.0 or higher, may have a very high positive predictive value in certain settings. But that does not mean every positive should be read in isolation.
If you are trying to sort through options, this breakdown of the Lyme disease tests can help you compare next steps.
Action step: If your ELISA is positive, ask: “What confirmatory test are you ordering, and when will I get it?” Get the answer before you leave the visit.
A negative result can mean no detectable antibodies at that time. It can also mean the test was done too early, the immune response was delayed, or the case is clinically more complicated.
This is where patients often feel gaslit. They know something changed. Their energy dropped. Their thinking slowed. Their joints started moving like rusty hinges at 6 a.m. But one negative screen gets treated like the last word.
It should not be the last word if:
Symptoms fit Lyme disease
Tick exposure is plausible
A rash was present
Illness started after outdoor exposure
Neurologic, joint, or heart symptoms are evolving
Action step: Bring a written symptom timeline to your next appointment. Keep it to one page. List dates, exposures, rashes, fevers, and new symptoms.
Our guide on tick disease blood test is a helpful resource outlining what it checks for, what it can detect, and what the results mean.
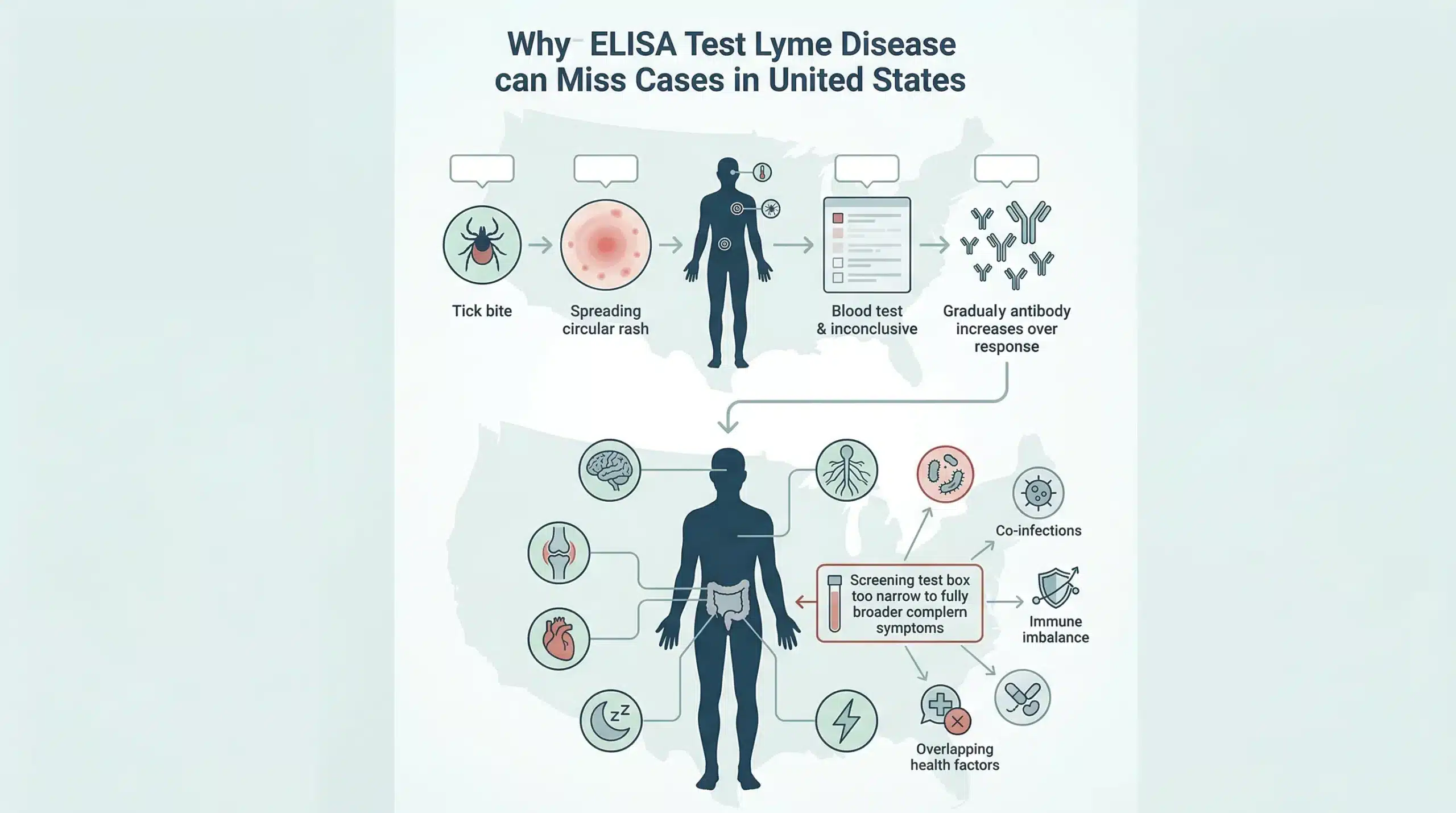
The ELISA test may miss Lyme disease most often in early infection and in more complex, multi-system cases. This is the part many suffering patients wish someone had explained sooner.
I’ve worked with many people who were told, “Your test was negative, so there’s nothing here,” while their bodies told a very different story.
Early infection is the classic blind spot. Antibodies may not be detectable yet, especially in the first days to few weeks after a bite.
This is why a person with a recent tick bite, a spreading rash, sweats, chills, neck pain, and crushing fatigue can still have a negative ELISA. The immune system simply may not have produced enough measurable antibodies yet.
If you had erythema migrans, many clinicians would treat based on that rash alone because it is so strongly associated with Lyme. Waiting for the blood test to “catch up” can waste time.
Action step: If symptoms started within the past month, ask whether your case should be judged more by clinical signs and exposure than by one early lab result.
This is where medicine gets harder. Some patients do not show up with the textbook story. They show up with brain fog, migrating pain, dizziness, sleep disruption, anxiety, palpitations, numbness, gut issues, or severe fatigue.
In these cases, a simple yes-no reading from one screening test may not capture the full picture. Persistent symptoms can reflect Lyme, co-infections, immune disruption, mold illness, or several overlapping problems at once. On our side of care, we often have to step back and ask a more useful question: what pattern explains the whole patient?
Action step: If your symptoms affect more than one body system, write them in groups: brain, nerves, joints, heart, gut, sleep, hormones. That takes 10 minutes and helps your clinician see the pattern faster.
The ELISA test fits into a broader Lyme evaluation as one tool, not the whole toolbox. Good Lyme assessment uses labs, yes. But it also uses symptoms, exposure history, physical clues, and clinical judgment.
This matters because Lyme is a pattern-based illness. You do not diagnose a pattern by staring at one number alone.
A strong Lyme workup starts with three questions:
What symptoms are present?
Was there likely tick exposure?
Does the timeline fit?
Doctors should ask about rash, flu-like onset, migrating joint pain, facial weakness, headaches, tingling, palpitations, memory problems, and profound fatigue. They should also ask where you have been: camping, gardening, dog walking, hunting, or hiking around brushy trails and creek beds.
In and around Austin, that can include greenbelt areas, Hill Country day trips, and backyard exposure that people often underestimate.
Clinical judgment matters most when the story is strong but the test is weak. That does not mean guessing. It means weighing evidence like a skilled investigator.
Action step: Create a one-page exposure history today. List travel, outdoor activity, tick bites, rashes, and when symptoms began.
If the ELISA result does not settle the case, clinicians may consider other tests. The right choice depends on stage of illness, symptoms, and what question you are trying to answer.
Possible next steps may include:
Western blot or another confirmatory immunoblot
Modified two-tier testing (MTTT)
PCR in selected situations
Other focused labs based on the full case
No single test solves every Lyme question. That is why test selection matters. A useful resource is this guide on test for tick-borne diseases in humans, outlining common symptoms and what tests to ask for when you suspect Lyme or other diseases carried by ticks.
Action step: Ask your clinician, “What exact question does the next test answer?” If they cannot answer that clearly, pause before spending more money.
If you suspect Lyme but your ELISA is negative, do not stop at the lab slip. Start with a structured next-step plan.
Here is the step-by-step approach I would want any patient to follow:
Review the timing of the test. If testing happened within the first few weeks, antibodies may not have risen yet.
Document your symptom timeline. Include the first strange day, any rash, fever, aches, tingling, dizziness, or cognitive changes.
Write down exposure risks. Tick bite, pet exposure, hiking, yard work, camping, or travel to endemic areas all matter.
Ask about repeat testing in 2 to 4 weeks. This is especially important if symptoms began recently.
Request confirmatory or alternate testing when clinically appropriate. That may include Western blot, MTTT, or other targeted labs.
Get a clinician who will look at the full picture. If your symptoms are multi-system, you need someone who can evaluate Lyme alongside mold, co-infections, immune stress, gut issues, and nervous system strain.
One hard truth: some patients lose months because they assume a negative ELISA means they should wait it out. I’ve seen people do that until the fatigue gets heavier, the insomnia gets worse, and they can no longer work a normal week. Please do not let one screening result silence what your body is saying.
For patients who need a wider lens, this resource on Lyme disease test can help you think through the next move.
Who this is for: people with a strong symptom pattern, possible exposure, or a rash history.
Who this is not for: people seeking emergency care for severe chest pain, fainting, stroke-like symptoms, or acute shortness of breath. Those need urgent evaluation now.
Action step: Spend 15 minutes today creating a folder with your labs, symptom notes, photos of any rash, and a list of questions for your next appointment.
The ELISA test for Lyme disease is useful, but it is only a screening tool. It measures antibodies, not the full reality of your illness. That means results must be read with timing, symptoms, exposure history, and clinical judgment.
If you have been told “it’s all in your head” because one ELISA came back negative, I want to say this plainly: you are not imagining your symptoms. Sequence matters. Context matters. And when the story fits, a deeper evaluation can change the course of care.
Start with your timeline. Gather your labs. Ask better questions. And if your current provider stops at one screening test, find one who will keep looking for the root cause.
References
John, T. M., & Taege, A. J. (2019). Appropriate laboratory testing in Lyme disease. Cleveland Clinic Journal of Medicine, 86(11), 751–759. https://doi.org/10.3949/ccjm.86a.19029
We have helped thousands of
people restore their health
and quality of life by diagnosing
and treating their Lyme Disease.
“Dr. Mueller’s approach to medicine is refreshing! There is only so much you can do with western medicine and in my life I was needing a new approach. By addressing the whole body, nutritional diet factors, environmental factors, blood work, and incorporating ideas I had not previously known, I was able to break through with my conditions. I am not only experiencing less pain in my life, but through the process of healing guided by Dr. Diane Mueller, I am now happy to say I have more consciousness surrounding how I eat, what to eat and when things are appropriate. Living by example Dr. Mueller has a vibrancy that makes you want to learn and know more about your body and overall health. I highly recommend her to anyone looking for new answers, a new approach to health, or in need of freedom from pain and limitations.”
-Storie S.
Kihei, HI