


Written by Dr. Diane Mueller
Tick-borne disease diagnosis often starts with a bad feeling that something is off. You feel sick, tired, dizzy, inflamed, or strangely unlike yourself, but the lab report says “normal,” and the story stops there.
It should not. In my experience working with complex Lyme and mold cases, this is where the real investigation begins. Tick-borne illnesses can hide behind vague symptoms, missed rashes, early false negatives, and co-infections that muddy the picture. If you have been told it is stress, aging, or “all in your head,” this guide will show you how diagnosis actually works and what to do next.
Tick borne disease diagnosis starts with clinical suspicion based on symptom patterns and exposure history, not just lab tests.
Early Lyme disease tests can be negative, so timing matters and repeat testing may be necessary to confirm diagnosis.
Symptoms like unexplained fatigue, joint pain, brain fog, and fever after outdoor exposure should raise suspicion for tick borne diseases.
Co-infections and overlapping health issues can complicate diagnosis, requiring broader testing beyond standard Lyme serology.
Organizing a detailed symptom timeline and previous test records helps clinicians identify patterns and make accurate diagnoses.
Negative test results do not always rule out tick borne diseases; persistent symptoms warrant further clinical evaluation and comprehensive testing.
We have helped thousands of people in Colorado, Wyoming, New Jersey, Pennsylvania, Texas, Wisconsin restore their health and quality of life by diagnosing and treating their Lyme Disease.
Here is the key fact: tick-borne diseases diagnosis is clinical first and laboratory-supported second. Good clinicians do not stare at one negative test and stop thinking.
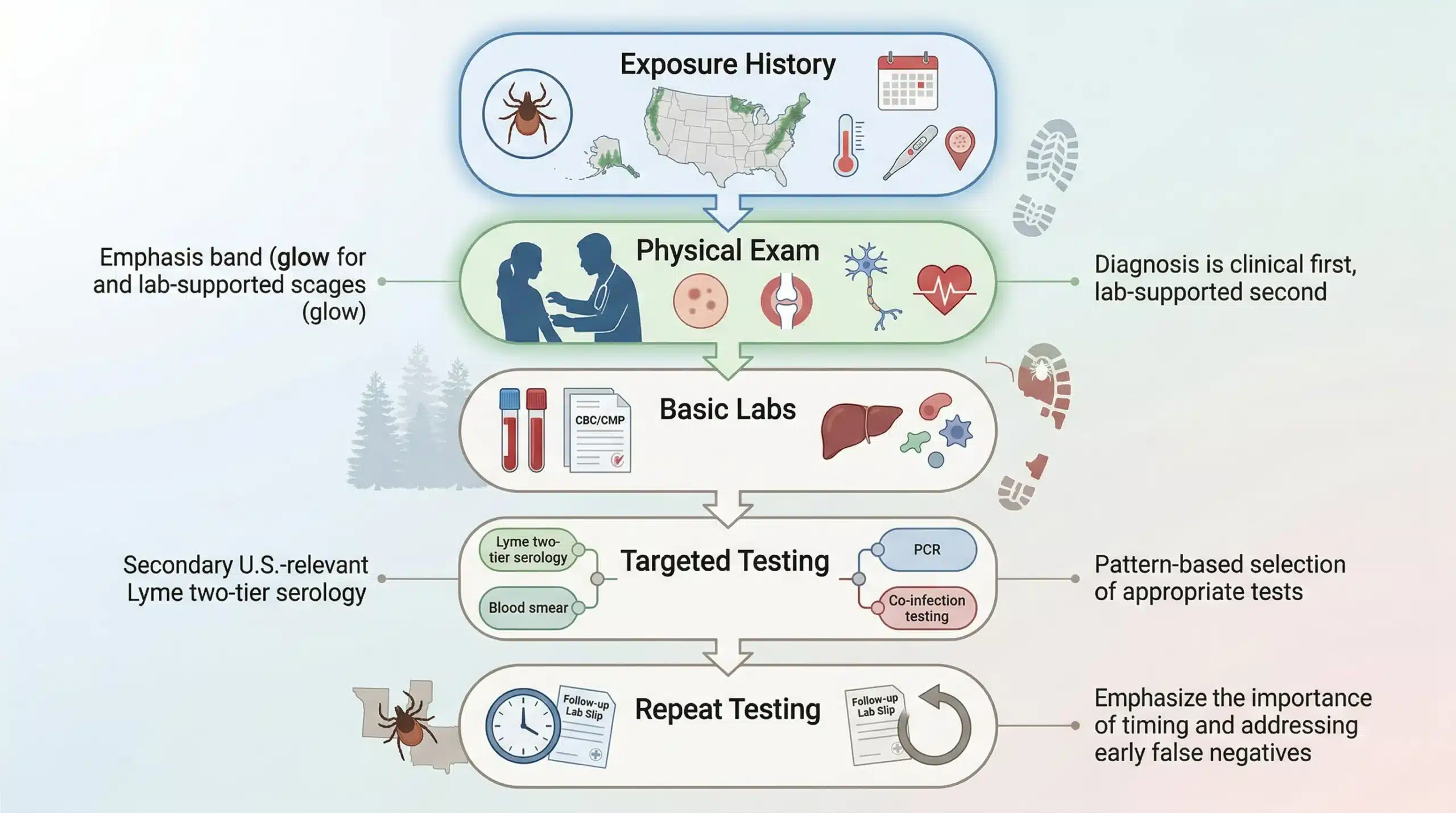
The usual process looks like this:
History: tick exposure, geography, season, rash, fever, and symptom timeline
Physical exam: rash, joint findings, nerve signs, heart rate changes
Basic labs: CBC, CMP, liver enzymes, inflammatory markers
Targeted testing: Lyme serology, PCR, blood smear, or co-infection panels based on the pattern
Repeat testing when timing matters: especially if the first test was too early
For Lyme, standard diagnosis often uses two-tier serology. For ehrlichiosis, anaplasmosis, or RMSF, paired antibody testing may help, but severe cases may need treatment before results return. Babesiosis may require PCR or a blood smear because antibody testing alone can miss active infection.
If you want a more detailed breakdown, read our guide on Lyme Disease Diagnosis. It discusses test timing, symptom pattern, and exposure history, not just a yes-or-no lab line. For difficult cases, choosing the best Lyme disease test approach depends on whether you need early detection, immune response data, or direct organism testing.
Do this today: ask for the exact name and date of every prior test. Put them in one folder. Give yourself 20 minutes.
Standard testing helps, but it is strongest when used at the right time. That is the part many people never hear.
What standard tests do well:
They can confirm infection after antibodies rise
PCR can detect genetic material in some cases
Blood smear can catch visible organisms like babesiosis in the right window
Paired tests can show a meaningful rise in antibodies over time
Where they fall short:
Early Lyme tests can be negative in the first few weeks
Low organism levels can produce false negatives
Cross-reactivity can confuse interpretation
One test often does not rule out co-infections
The research base in the National Library of Medicine has documented these timing limits for years. Even mainstream patient education sources such as WebMD acknowledge that Lyme and related infections can be hard to confirm early.
That is why many patients end up cycling through repeat visits without answers. A better Lyme disease test plan matches the method to the stage of illness. Sometimes the first negative means “too soon,” not “case closed.”
Do this today: review whether your test was done within the first 2 to 4 weeks of symptoms. If yes, ask whether repeat testing is appropriate.
We have helped thousands of people in Colorado, Wyoming, New Jersey, Pennsylvania, Texas, Wisconsin restore their health and quality of life by diagnosing and treating their Lyme Disease.
This is where many chronic cases get messy fast. One tick can carry more than one infection, and one illness can expose other weak points in the body.
A patient may have Lyme plus babesiosis, or Lyme plus anaplasmosis. That changes the symptom picture. Babesiosis often brings night sweats, shortness of breath, and a “can’t get a full breath” feeling. Bartonella can bring foot pain, irritability, anxiety, and nerve symptoms. If you test for only one infection, you can miss the real story.
Then there are overlapping root causes. Mold exposure, gut dysfunction, thyroid issues, hormone shifts, and nervous system strain can all amplify symptoms. In my clinic work, sequence matters. If the body is dealing with infection and mold toxins, the patient may not respond as expected until both are addressed.
A broader strategy like Co-Infections Testing for Lyme can help when symptoms do not fit a single diagnosis. And if you are sorting through options, a smarter Lyme Disease Test: choice often includes more than a standard two-tier Lyme screen.
Do this today: list any mold exposure, water damage, past mono, major stress, or hormone changes next to your symptom timeline. Give it 15 minutes.
A negative test does not always end the case. If symptoms persist and the pattern fits, you need a next-step plan.
Start here:
Check timing: Was testing done too early?
Retest if needed: paired serology or PCR may add useful data
Ask about co-infections: especially with sweats, air hunger, nerve pain, or unusual psychiatric symptoms
Review routine labs: CBC and liver enzymes can offer clues
Look at the whole body: mold, gut issues, thyroid, iron, sleep, and nervous system load can all shape symptoms
Find a clinician who treats clinically, not only by one lab result
I say this with care and honesty: not every chronic symptom is Lyme. But not every negative Lyme test rules Lyme out either. That tension is real. Patients in Connecticut, from Stamford to Mystic, often spend years bouncing between specialists before someone finally connects the dots.
If your case is stalled, resources on best Lyme disease test options and more advanced co-infections testing can help you ask better questions. For many people, the turning point is not one magic lab. It is a smarter workup.
Do this today: book one focused appointment with all records, your timeline, and your top three questions. Plan 30 minutes to prepare.
Tick-borne disease diagnosis is often missed because symptoms overlap, tests have timing limits, and co-infections change the picture. But missed does not mean impossible.
If your symptoms do not add up, stop guessing and start organizing the evidence. Build your timeline, review test timing, and work with a clinician who will look for root causes instead of dismissing the pattern. That step can change everything.
Tick-borne diseases often present with vague symptoms like fatigue, fever, and headaches that mimic viral illnesses. Early antibody tests can be negative, and classic signs like the bull’s-eye rash appear in only about 70-80% of Lyme cases, making diagnosis challenging.
Early Lyme tests can be negative because antibodies take weeks to develop. Testing within the first 2 to 4 weeks of symptoms may not detect infection, so repeat testing later improves accuracy and helps confirm diagnosis.
New multi-system symptoms after potential tick exposure such as fever, chills, unexplained fatigue, joint pain, brain fog, rash, night sweats, and abnormal lab results should prompt evaluation for tick-borne diseases.
Diagnosis begins with clinical assessment including exposure history and symptom timeline, followed by physical exam and targeted tests like two-tier Lyme serology, PCR, blood smears, and co-infection panels to confirm infections.
Yes, testing for co-infections like babesiosis or anaplasmosis is important because ticks can transmit multiple pathogens that complicate symptoms and treatment, requiring broader panels for accurate diagnosis.
If symptoms persist with suspicion for tick-borne illness, consider retesting after the appropriate interval, testing for co-infections, review other health factors, and seek a clinician who bases diagnosis on clinical assessment, not just labs.
We have helped thousands of
people restore their health
and quality of life by diagnosing
and treating their Lyme Disease.
“Dr. Mueller’s approach to medicine is refreshing! There is only so much you can do with western medicine and in my life I was needing a new approach. By addressing the whole body, nutritional diet factors, environmental factors, blood work, and incorporating ideas I had not previously known, I was able to break through with my conditions. I am not only experiencing less pain in my life, but through the process of healing guided by Dr. Diane Mueller, I am now happy to say I have more consciousness surrounding how I eat, what to eat and when things are appropriate. Living by example Dr. Mueller has a vibrancy that makes you want to learn and know more about your body and overall health. I highly recommend her to anyone looking for new answers, a new approach to health, or in need of freedom from pain and limitations.”
-Storie S.
Kihei, HI