
Quick Answer: Lyme disease recovery time depends on stage, duration of infection, co-infections, and whether conditions like mold illness are also present. Acute Lyme caught within weeks may resolve in 2-4 weeks with treatment. Early disseminated cases often take 2-6 months. Late or chronic Lyme typically requires 12-24 months of comprehensive, phased care. Recovery is rarely linear: herxing, setbacks, and partial windows of improvement are part of the process, not signs of failure. What matters is matching treatment to stage and addressing all contributing factors, not just the Lyme bacterium.
Key Takeaways
- Lyme disease recovery time ranges from weeks (acute, early-caught) to 1-2 years or more (late-stage, co-infected, or mold-overlap cases). There is no universal answer.
- The biggest variables are how long the infection was missed, which co-infections are present (Bartonella, Babesia, Ehrlichia), and whether mold or CIRS exposure is adding a separate inflammatory burden.
- Recovery is not linear. Herxheimer reactions (temporary worsening during treatment), setbacks, and “two steps forward, one step back” are clinically normal, not signs of failure.
- “Still sick after antibiotics” does not mean incurable. It may mean untreated co-infections, PTLDS, or an overlapping condition that was not addressed.
- Functional milestones (sleep quality, cognitive stamina, exercise tolerance) give a clearer picture of progress than symptom-free days alone.
- Working with a Lyme disease specialist who understands the full picture, including co-infections and mold, is the most reliable way to shorten the timeline.
The real question beneath every search about Lyme recovery timelines is: how much longer is this going to take?
Honest specialists will not give you a single number. The answer depends on variables specific to each patient: how long the infection was missed, whether co-infections are present, whether mold or CIRS is adding a parallel inflammatory burden, and whether the nervous system has become sensitized after years of chronic illness.
What follows is a stage-based framework and the variables that move the timeline in either direction.
Why There Is No Single Lyme Disease Recovery Timeline
The stages of Lyme disease represent different clinical pictures with different recovery trajectories. Borrelia burgdorferi can remain localized or disseminate throughout the body over weeks to years, and “recovery” means different things to different patients: symptom-free, functional enough to work and exercise again, or managing a chronic condition rather than being disabled by it. The timeline to each endpoint differs.
What clinical research does confirm is that a subset of patients experience persistent symptoms after treatment, and the severity ranges widely from mild to disabling. A 2020 review in Frontiers in Medicine characterized these persistent symptoms and the several mechanisms still under study to explain them, including immune dysregulation and altered neural signaling (Rebman and Aucott, 2020). In my clinical experience, the longer an infection stays active before treatment begins, the more the recovery curve tends to extend.
Stage-by-Stage Recovery Timeline
Acute Lyme Disease (Caught Early)
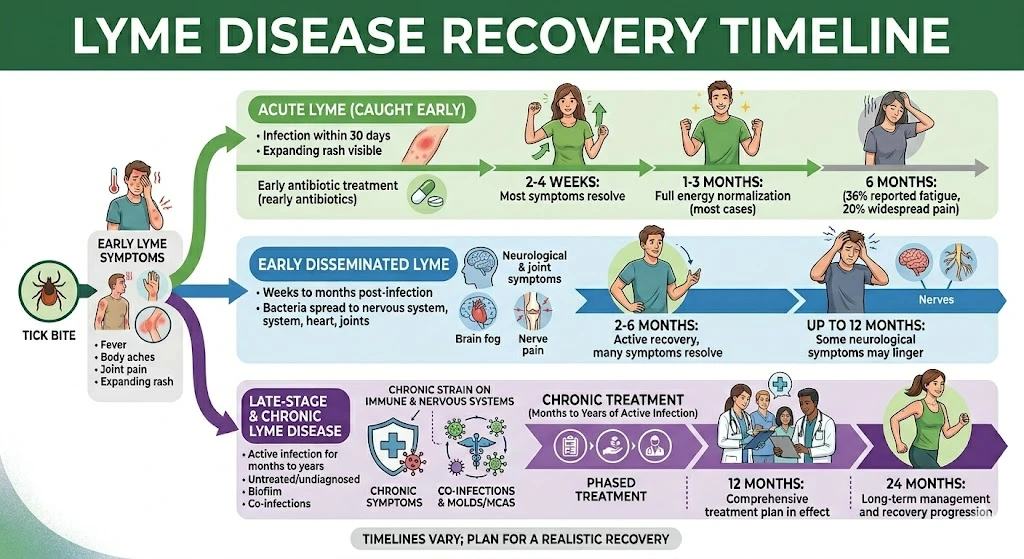
Acute Lyme is infection caught within 30 days of the tick bite, often with the classic expanding rash still visible. With appropriate antibiotic treatment, most patients see resolution of primary symptoms within 2-4 weeks, with full energy normalization typically within 1-3 months in otherwise healthy patients with no co-infections.
The qualifier: “most” is not “all.” In one prospective cohort that followed patients after treatment, a meaningful share reported persistent symptoms at six months, including 36% with fatigue and 20% with widespread pain (Aucott et al., 2013).
Early Disseminated Lyme (Weeks to a Few Months After Infection)
Early disseminated Lyme occurs when the bacteria spread into the nervous system, heart, or multiple joints. Neurological symptoms, including cognitive difficulties and nerve pain, can take months to resolve even after appropriate treatment. Most patients in this category can expect 2-6 months of active recovery, though some neurological symptoms may take up to 12 months to settle.
The contrast between acute and chronic Lyme disease matters here: early disseminated is still technically acute, but it introduces complexity that characterizes harder-to-treat cases.
Late-Stage and Chronic Lyme Disease (Months to Years of Active Infection)
Late-stage Lyme refers to infection active, often undiagnosed, for months to years. By this point the bacteria may have established biofilm colonies, co-infections are frequently present, and the immune and nervous systems have been under chronic strain.
A realistic recovery timeline here is 12-24 months of comprehensive, phased treatment. That is a number to plan around, not be discouraged by. Late-stage Lyme disease treatment requires more attention to co-infections, immune dysregulation, detoxification pathways, and overlapping conditions like mold illness or MCAS.
[ADD IMAGE: lyme-disease-treatment-phases-diagram.jpg | Alt: “Illustration of how chronic Lyme disease treatment typically progresses in stages over time, from reducing infection load to nervous system recovery”]
The Variables That Move the Timeline
Duration Before Diagnosis
Every year of undiagnosed infection adds complexity: more established biofilm colonies, greater immune dysregulation, more nervous system strain. Patients who went 5-10 years without a diagnosis should plan for a longer timeline than someone diagnosed at 6 months. That is honest, not hopeless.
Co-Infections
Lyme disease rarely travels alone. The same ticks that carry Borrelia burgdorferi also carry Bartonella, Babesia, Ehrlichia, and other organisms that require different treatment approaches. When co-infections are present and untreated, targeting Lyme alone will not produce full recovery. Bartonella is known for psychiatric manifestations (anxiety, rage episodes) often misattributed to Lyme alone. Babesia presents with sweats, air hunger, and cyclical fatigue. Each adds a treatment component and additional time.
Mold and CIRS Overlap
Chronic Inflammatory Response Syndrome (CIRS) caused by mold exposure creates a parallel inflammatory burden that makes Lyme treatment harder to tolerate and less effective. Research by Dr. Ritchie Shoemaker documented that patients exposed to water-damaged buildings show distinct patterns of immune dysregulation that persist regardless of other treatment (Shoemaker et al., 2006). If your Lyme treatment keeps stalling, mold is worth evaluating. In my practice, patients who made no progress for two years began recovering once we addressed their CIRS load.
Herxheimer Reactions and Treatment Pacing
A Herxheimer reaction (“herxing”) is a temporary worsening of symptoms as bacteria die off during treatment. It is an expected part of recovery. Understanding Herxheimer reaction and detox phases helps patients stay on course when symptoms flare. Severe herxing may require slowing the treatment pace, which is appropriate clinical management, not failure. Pushing through without adjustment risks immune overwhelm.
Nervous System Sensitization
In patients who have been ill for years, the nervous system can enter a state of chronic alarm that persists after the bacterial burden is reduced, manifesting as disproportionate fatigue, sensory sensitivities, and the frustrating gap between improving labs and not feeling recovered. This is physiological, not psychological, and one of the last pieces to resolve.
What Realistic Milestones Look Like

When recovery is slow, progress can feel invisible. These are the milestones I watch for in clinical practice, roughly in order of appearance.
Months 1-3: Sleep quality improves before other symptoms shift. Herxheimer reactions become more predictable. Brief cognitive windows (brain fog lifts for short periods). Digestive function stabilizes.
Months 3-6: Fatigue becomes episodic rather than constant. Exercise tolerance increases. Mood stabilizes; fewer days of profound despair. Cognitive stamina extends.
In the second half of the first year (months 6-12), patients typically regain the ability to manage partial daily activities: cooking, light work, meaningful social engagement. Flares become shorter and less severe, lab markers begin to normalize, and most patients start distinguishing a "bad day" from a "Lyme day" for the first time.
By months 12-24, most late-stage patients on a comprehensive protocol have returned to a functional baseline. Active treatment gives way to maintenance support centered on diet, sleep, and stress management. Residual sensitivities remain, but they no longer govern daily life.
Tracking these milestones matters more than tracking symptom-free days. Recovery from chronic Lyme is cumulative, not a threshold you cross one morning.
Post-Treatment Lyme Disease Syndrome: When "Still Sick" Has a Name
If you completed antibiotics and still feel unwell, you may have been told your symptoms are no longer Lyme-related. The clinical reality is more complicated.
Post-treatment Lyme disease syndrome (PTLDS) is a recognized condition affecting a meaningful subset of patients. A 2022 prospective cohort study applying operationalized PTLD criteria found that people with a prior history of Lyme disease were roughly five times more likely to meet those criteria than those without, confirming PTLDS as a definable condition rather than a purely subjective complaint (Aucott et al., 2022). PTLDS is not the same as ongoing active infection, does not respond to additional rounds of the same antibiotics, and requires a different treatment approach. Two controlled trials of extended antibiotic treatment found no benefit over placebo for patients with persistent symptoms after standard treatment (Klempner et al., 2001).
The post-treatment Lyme disease syndrome page on this site covers diagnostic criteria and clinical features in detail.
For patients who feel stuck after standard treatment, the path forward involves evaluating co-infections that were never addressed, mold or CIRS overlap, and immune dysregulation that persists after the bacterial burden is reduced. The approach to Lyme disease treatment at this practice is built around that kind of comprehensive re-evaluation.
How to Track Your Own Progress
When recovery spans 12-24 months, subjective day-to-day experience is not a reliable guide.
Symptom scoring at intervals: Rate 5-8 core symptoms on a 1-10 scale at the start of treatment and every 4-8 weeks. Individual days will vary; the trend line is what matters.
Functional capacity tracking: Can you walk further than three months ago? Sleep 6 hours without waking? Hold a conversation without losing your train of thought? Functional markers move more predictably than symptom intensity.
Lab retesting: Inflammatory markers, co-infection titers, and HPA axis markers should be retested every 3-6 months. Labs improving before symptoms fully resolve is common and a reliable leading indicator.
The chronic Lyme disease treatment protocols at this practice include structured milestone tracking from the beginning.
The Non-Linear Reality: What Nobody Warns You About
Every patient I have worked with who recovered from late-stage Lyme went through the same pattern: progress, setback, more progress, another setback, then a longer sustained window of improvement. The setbacks were not treatment failures. They were part of the biology.
Herxing, immune challenges from ordinary illness, treatment adjustments, re-exposures to mold: all create temporary regressions. A patient who reads a Lyme disease recovery story and sees “I recovered in 18 months” rarely sees the months when that patient thought they were getting worse.
What keeps people on course is not optimism. It is a framework for understanding what is happening and a clinical team who can distinguish a meaningful setback from a temporary regression. The question “is this normal?” is one I answer many times a week. For most patients in active treatment, the honest answer is yes.
Frequently Asked Questions
Acute Lyme treated within weeks of infection may resolve in 2-4 weeks. Early disseminated cases typically take 2-6 months. Late or chronic Lyme, particularly with co-infections or mold overlap, usually requires 12-24 months of comprehensive, phased treatment. There is no universal number because the variables differ significantly between patients.
If your Lyme went undiagnosed for more than a few months, plan for recovery measured in months, not weeks. Functional milestones (sleep, cognitive stamina, exercise tolerance) typically move before you feel “normal” again. Patients with late-stage disease following a comprehensive protocol often reach meaningful functional recovery by 12-18 months, with continued improvement through month 24.
Persistent symptoms after standard antibiotics may reflect PTLDS, untreated co-infections (Bartonella and Babesia are commonly missed), ongoing mold or CIRS exposure, or immune dysregulation that outlasts the bacterial burden. A comprehensive re-evaluation with a Lyme-literate specialist is the appropriate next step. Read more about what happens after Lyme disease treatment and what to do next.
Many patients achieve full functional recovery, particularly when Lyme is caught early. For late-stage or chronic Lyme, “full recovery” most often means returning to a normal daily life while maintaining certain supportive habits. Clinical studies document significant, measurable improvement in patients who receive stage-matched treatment. The phrase “Lyme will always be something I consider” captures the realistic picture more accurately than either “complete cure” or “permanent disability.”
The four biggest factors are: delayed diagnosis, active co-infections that were never treated, concurrent mold or CIRS exposure, and nervous system sensitization after years of chronic illness. Addressing all four, not just the Lyme bacterium, is the difference between treatment that works and treatment that partially works.
A Herxheimer reaction is a temporary worsening of symptoms as bacteria die off during treatment. It is an expected part of recovery, not a sign treatment is failing. Severe herxing may slow the treatment pace and extend the active phase by weeks to months. Managing it appropriately, rather than pushing through without adjustment, protects the overall recovery trajectory.
"I Just Want My Life Back": Let's Figure Out What's in the Way
If you have been sick for years and prior treatment has not gotten you where you hoped, a comprehensive evaluation can identify what has been missed. Dr. Mueller’s practice serves patients via telehealth in CO, WY, NJ, PA, TX, and WI.
Book an Initial Consultation – $300
Telehealth. No referral needed. Comprehensive intake before your first visit.
Author: Dr. Diane Mueller, ND, LAc, DAOM
Medical Disclaimer: The information in this article is intended for educational purposes only and does not constitute medical advice, a diagnosis, or a treatment recommendation. Lyme disease recovery is highly individualized and depends on clinical factors that vary from patient to patient. Do not begin or discontinue any treatment based solely on the information presented here. If you are experiencing symptoms described in this article, consult a licensed healthcare provider experienced in tick-borne illness and complex chronic conditions.

