


Quick Answer: Bartonella testing is unreliable by design: the bacteria hides inside cells, alters its surface proteins to evade immune detection, and circulates intermittently. Standard IFA antibody tests run by most labs check for only one or two Bartonella species and routinely return negative even in confirmed infections. A negative result does not rule out Bartonella. More sensitive options exist through specialty labs (Galaxy Diagnostics, IGeneX) using ddPCR, FISH, and culture-enhanced methods. When symptoms match and testing is negative, experienced clinicians often treat based on the clinical picture.
If your Bartonella test came back negative but your symptoms are an exact match, that result does not mean you don’t have it. It may mean the test wasn’t sensitive enough to catch it.
This is one of the most common and most damaging misunderstandings I see in practice. Patients are told “tested negative, you’re clear,” go years without a diagnosis, and continue getting sicker. The problem isn’t the patient. The problem is that standard Bartonella tests are designed for a more straightforward infection than Bartonella actually is.

The core problem is biology, not lab quality.
Bartonella survives through active evasion: not by overwhelming the immune system, but by hiding from it. Three mechanisms explain most of the false negatives:
Bartonella takes up residence inside red blood cells (erythrocytes) and the cells that line blood vessels (endothelial cells). Antibody tests look for immune proteins circulating in the blood; they cannot detect bacteria that have retreated into host tissue. Published research confirms that Bartonella creates specialized compartments inside infected cells called Bartonella-containing vacuoles, which are designed to resist the cell’s normal destruction pathways (Source: Xi et al., Virulence 2024).
When the bacteria are inside cells, standard antibody testing may return negative even as the infection is active.
Bartonella uses a strategy called antigen variation: it alters the proteins displayed on its outer surface, making it harder for the immune system to maintain consistent antibody production. This is why the same patient can test negative one month and produce a different antibody pattern the next. It also explains why IFA titers can fluctuate and why a single low titer is not a clean “all clear.” (Source: Xi et al., Virulence 2024)
Bartonella does not maintain a constant presence in the bloodstream. It cycles in and out of the blood in waves, re-seeding the circulation in bursts. A blood sample drawn on the wrong day will not capture the bacteria even if it’s present. This intermittent bacteremia is a well-documented challenge in co-infections testing and one reason serial testing often finds what a single draw misses.
Most standard labs (Quest, LabCorp) run an IFA (indirect immunofluorescence assay) for antibodies against Bartonella henselae and Bartonella quintana only. There are more than 40 known Bartonella species, with a growing number documented as pathogenic to humans as detection improves (Source: Gutierrez et al., Vector Borne Zoonotic Diseases 2017). If you are infected with any other species, the standard panel will not detect it.
A negative standard result doesn’t mean you’re negative for Bartonella. It means you’re negative for those two species, using that method, on that day. Patients who acquire Bartonella through ticks may carry species and strains outside the standard clinical panel entirely.
For a look at how Bartonella symptoms compare with other tick-borne infections, that page covers the clinical patterns that should trigger a workup.
Understanding what each test type detects helps you interpret results and have a more informed conversation with your provider.
IFA Serology (Indirect Immunofluorescence Assay): IFA is the most widely available Bartonella test. It measures antibodies (IgG and IgM) the immune system has produced in response to Bartonella. A positive IFA indicates past exposure and immune response; it does not confirm active infection. Elevated IgG titers can persist for months to years after a resolved infection. Published review of Bartonella laboratory diagnostics notes that IFA requires appropriate antigen preparation and clinical interpretation to be useful (Source: Agan & Dolan, Clinical Laboratory Medicine 2002).
PCR (Polymerase Chain Reaction): PCR detects Bartonella DNA directly in blood. A positive result is strong evidence of active infection. The critical limitation: PCR requires bacteria to be present in the sample at the exact time of collection. Given Bartonella’s intermittent bacteremia, a single negative PCR is not a clean all-clear. Targeting conserved genomic loci such as the riboflavin synthase gene (ribC) improves species-level identification from clinical specimens (Source: Drancourt et al., 2003). Combining PCR with serology improves sensitivity significantly compared to either method alone (Source: Agan & Dolan, 2002).
ddPCR (Digital Droplet PCR): ddPCR is a more sensitive evolution of conventional PCR. Where standard PCR produces a yes/no signal, ddPCR partitions the sample into thousands of individual droplets and counts reactions digitally, allowing detection of very low bacterial loads that standard PCR misses. Galaxy Diagnostics integrates ddPCR with culture enrichment and serology in a combined panel designed for tick-borne Bartonella.
FISH (Fluorescent In-Situ Hybridization): FISH detects Bartonella nucleic acid directly within individual cells on a blood smear rather than in extracted blood, allowing visualization of organisms inside red blood cells. This matters because that is where Bartonella hides. IGeneX offers FISH as part of their panel. A positive FISH result on a smear is meaningful direct evidence of intracellular infection that serology and standard PCR cannot provide.
Culture: Growing Bartonella in culture is the most definitive confirmation that living bacteria are present, but also the least practical clinically. Bartonella is fastidious: it grows slowly, requires specific conditions, and takes weeks. Culture appears in some Galaxy Diagnostics enhanced panels and confirms viable organisms when positive.
ImmunoBlot: IGeneX’s Bartonella ImmunoBlot detects antibodies against multiple species on a single panel, with more resolution than a standard IFA. It provides band-level data similar to how a Lyme Western blot gives more nuance than ELISA, and is particularly useful when standard IFA titers are equivocal.
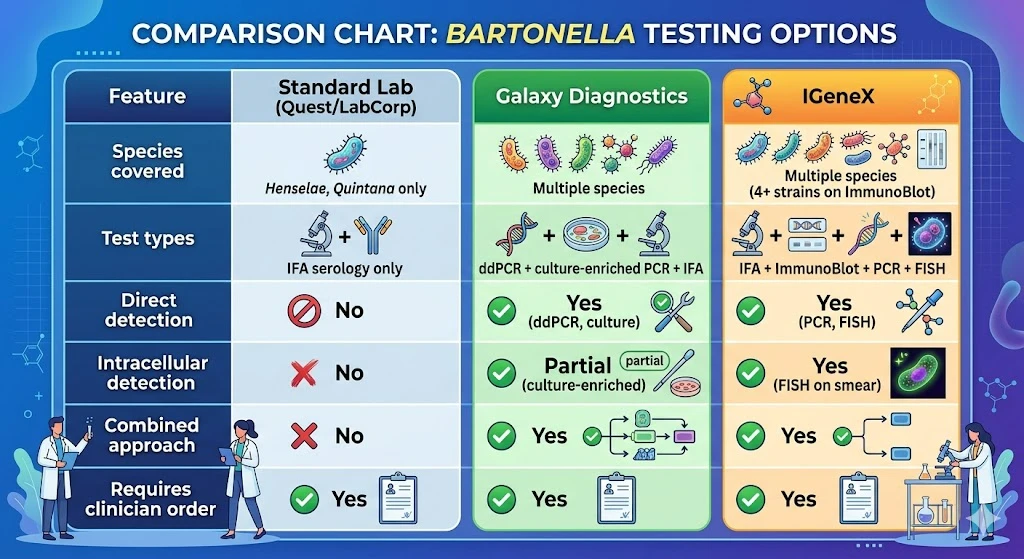
| Feature | Standard Lab (Quest/LabCorp) | Galaxy Diagnostics | IGeneX |
|---|---|---|---|
| Species covered | Henselae, Quintana only | Multiple species | Multiple species (4+ strains on ImmunoBlot) |
| Test types | IFA serology only | ddPCR + culture-enriched PCR + IFA | IFA + ImmunoBlot + PCR + FISH |
| Direct detection | No | Yes (ddPCR, culture) | Yes (PCR, FISH) |
| Intracellular detection | No | Partial (culture-enriched) | Yes (FISH on smear) |
| Combined approach | No | Yes | Yes |
| Requires clinician order | Yes | Yes | Yes |
Published guidelines recommend real-time PCR as a primary screening tool followed by confirmatory molecular assays, with culture where feasible to confirm viable organisms. (Source: Gutierrez et al., Vector Borne Zoonotic Diseases 2017) Standard labs don’t offer that approach. Specialty labs do.
A positive IFA or ImmunoBlot means your immune system has been exposed to Bartonella; it does not confirm active infection, since antibody titers can persist for years after a resolved infection. A positive PCR or ddPCR means Bartonella DNA was present in your blood at the time of the draw: stronger evidence of current infection. A positive FISH result, which visualizes organisms inside cells, carries significant clinical weight. The combination that provides the most confidence is positive direct detection (PCR, FISH, or culture) alongside compatible symptoms and supportive serology.
A negative result means bacteria were not detected in this sample at this time using this method. Bartonella DNA was still detected in 19% of patients with Lyme-like illness in a 2024 dry blood spot study, confirming that co-infection rates are meaningful even when standard testing returns negative. (Source: Beard et al., Microorganisms 2024)
When symptoms are consistent, see our co-infection symptom comparison for clinical patterns. An experienced clinician may recommend treatment based on the full picture even when testing is equivocal.
In tick-borne illness, the clinical picture and testing work together to make a diagnosis, not testing alone. The characteristic Bartonella symptom cluster includes anxiety or rage disproportionate to circumstance, unusual stretch marks (striae) in locations not explained by weight gain, burning pain on the soles of the feet, and a distinctive skin rash that differs from the Lyme bull’s-eye. Accompanied by tick exposure history or a confirmed Lyme diagnosis, this picture warrants evaluation even when initial testing returns negative.
For the full symptom picture that should trigger testing, see our page on Bartonella and Lyme co-infection.
Bartonella, Lyme (Borrelia burgdorferi), and Babesia share tick vectors and are frequently co-transmitted. Testing for all three at initial evaluation is more efficient than testing sequentially, and it changes the treatment approach: Bartonella requires different antimicrobial agents than Borrelia. Treating Lyme alone in a patient who also carries Bartonella typically produces incomplete improvement, and the reason often goes unidentified for years.
A 2024 dry blood spot study confirmed that Bartonella co-infection rates are meaningful even in patients whose standard testing returned negative. (Source: Beard et al., 2024)
For how these three infections present differently, see our Babesia vs. Bartonella vs. Lyme overview.
Most primary care physicians order standard IFA serology if they order anything. Useful questions to bring: Which species does this panel cover? Is there a direct detection option (PCR, FISH)? Can we run a co-infection panel for Bartonella, Borrelia, and Babesia together? A provider familiar with the diagnostic limitations will take these seriously. If you’re not getting answers, a Lyme disease specialist with co-infection experience can interpret both the lab data and the clinical picture together.
No single test is definitive. The most thorough approach combines methods: specialty labs (Galaxy Diagnostics, IGeneX) offer broader species coverage and higher-sensitivity detection through ddPCR, FISH, and culture-enhanced PCR that standard labs don’t provide. Positive direct detection (PCR, FISH) carries more diagnostic weight than positive antibodies alone. A negative panel does not rule out infection.
Yes. Bartonella hides inside cells where antibody tests cannot reach, circulates intermittently in the bloodstream, and varies its surface proteins to evade consistent antibody production. False negatives occur on even well-run panels. Clinicians experienced in tick-borne illness often treat based on the clinical picture when testing is negative but symptoms are consistent.
Standard labs (Quest, LabCorp) run IFA serology for Bartonella henselae and quintana only. Galaxy Diagnostics provides ddPCR, culture-enhanced PCR, and serology combined. IGeneX offers IFA, ImmunoBlot, PCR, and FISH. Specialty options cover more species and use detection methods with higher sensitivity for low-level or intracellular infection.
Often, yes. The characteristic pattern (neuropsychiatric symptoms, striae, foot pain, tick or flea exposure history) alongside Lyme co-infection context provides the basis for clinical diagnosis when testing cannot confirm it. Published guidelines recognize that laboratory results alone have important limitations in this context.
Standard IFA serology returns in 5-10 business days. Specialty panels through Galaxy Diagnostics or IGeneX typically take 2-4 weeks because culture-enhanced and FISH methods require longer processing. Results need to be interpreted in clinical context at a follow-up appointment; the numbers alone rarely tell the full story.
Yes. Bartonella, Lyme, and Babesia share tick vectors and are frequently co-transmitted. Co-infection panels allow all three to be assessed from a single blood draw, and knowing which infections are present shapes the treatment protocol from the start since Bartonella requires different agents than Borrelia.
A negative Bartonella test is not the final word. If your symptoms fit and your current provider isn’t digging deeper, a specialist who understands the full co-infection picture can order the right tests and interpret results in context. My practice serves patients in CO, WY, NJ, PA, TX, and WI via telehealth.
Book an Initial Consultation – $300
Telehealth. No referral needed. Comprehensive intake before your first visit.
Written by Dr. Diane Mueller, ND, LAc, DAOM
Medical Disclaimer: The information in this article is intended for educational purposes only and does not constitute medical advice, a diagnosis, or a treatment recommendation. Bartonella testing and co-infection evaluation are complex medical matters requiring individualized assessment by a qualified clinician. Do not begin or discontinue any treatment based solely on the information presented here. If you are experiencing symptoms described in this article, consult a licensed healthcare provider experienced in tick-borne illness.