


Quick Answer: CIRS treatment follows the Shoemaker protocol, a sequential framework that begins with removing biotoxin exposure, uses bile acid sequestrants to clear mycotoxins, eradicates MARCoNS nasal colonization, restores depleted hormones (MSH, VIP), and corrects the inflammatory cascade. A 2024 systematic review confirmed the Shoemaker protocol is the only CIRS treatment with documented clinical efficacy. The sequence is non-negotiable: skipping or reordering steps produces poor outcomes. For the 25% of people with HLA-DR genetic susceptibility, structured specialist-guided treatment is required. The body will not clear the biotoxin burden on its own.
You moved out of the moldy house. Your labs show nothing dramatic. And you still feel terrible: brain fog, fatigue, air hunger, the sense that something is still very wrong. There is a reason it hasn’t resolved, and it has nothing to do with willpower or anxiety.
I have treated CIRS for years, and I had Lyme disease myself. CIRS is real, it is testable, it is treatable, and the reason most treatment fails is not the protocol. It’s the sequence.
CIRS is a multi-system biotoxin illness driven by the innate immune system’s inability to clear mycotoxins from water-damaged buildings and biotoxins from Lyme disease, algae, and certain bacteria. The resulting inflammatory state disrupts hormonal pathways, suppresses regulatory neuropeptides, and produces a symptom picture so broad that most clinicians don’t recognize it as a single condition.
Standard workups (CBC, metabolic panel, thyroid) come back normal. The patient is told it’s stress. Years pass.
In an estimated 25% of the population, according to Shoemaker’s published research, specific HLA-DR gene variants prevent the immune system from tagging mycotoxins for clearance. Instead of being excreted, biotoxins recirculate through enterohepatic cycling, depositing in fatty tissues including the brain, and driving sustained immune activation with no identifiable foreign pathogen. Standard labs miss it because they are not looking in the right place.
The CIRS symptoms page covers the full diagnostic picture.
The Shoemaker protocol is the only structured CIRS treatment approach with documented clinical efficacy. A 2024 systematic review in Annals of Medicine and Surgery examined 13 CIRS treatment studies and found the Shoemaker protocol in 11 of them, the only approach that produced statistically significant improvement in objective biomarkers and symptom resolution. (Dooley et al., 2024)
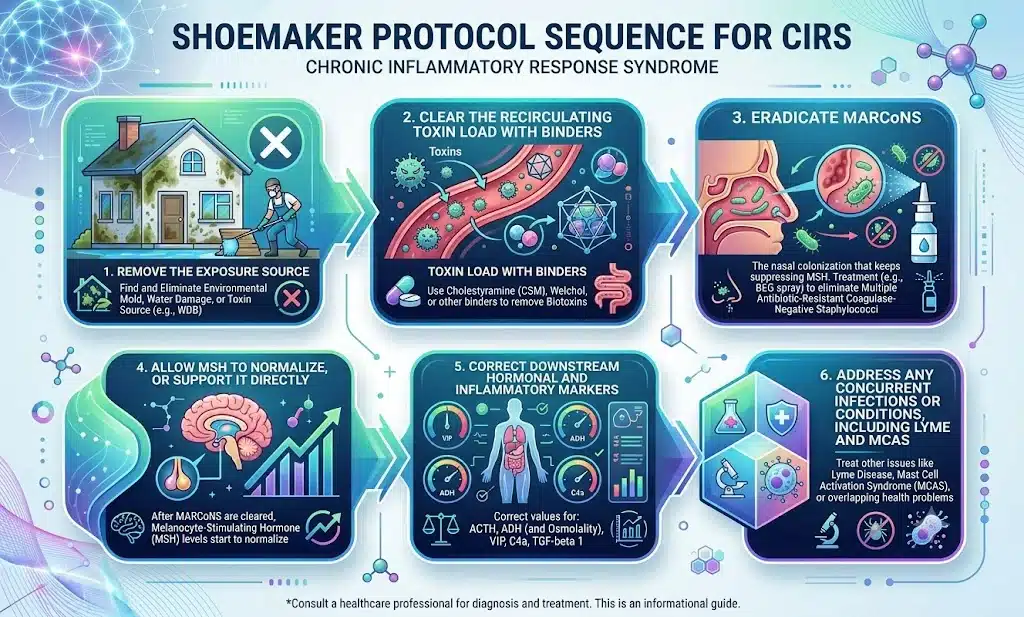
The protocol is sequential. The steps cannot be shuffled. Running VIP before clearing MARCoNS worsens the nasal colonization. Starting aggressive Lyme treatment before reducing the mycotoxin burden produces Herxheimer reactions an already-compromised immune system cannot handle.
Core sequence logic:
Step 6 is the one most CIRS practitioners skip. We’ll come back to it.
Nothing else works if the exposure continues. The first step is source identification: ERMI dust testing, professional mold inspection, and if necessary, temporary relocation during remediation.
Once exposure is addressed, we begin active toxin binding to interrupt the enterohepatic recirculation of mycotoxins.
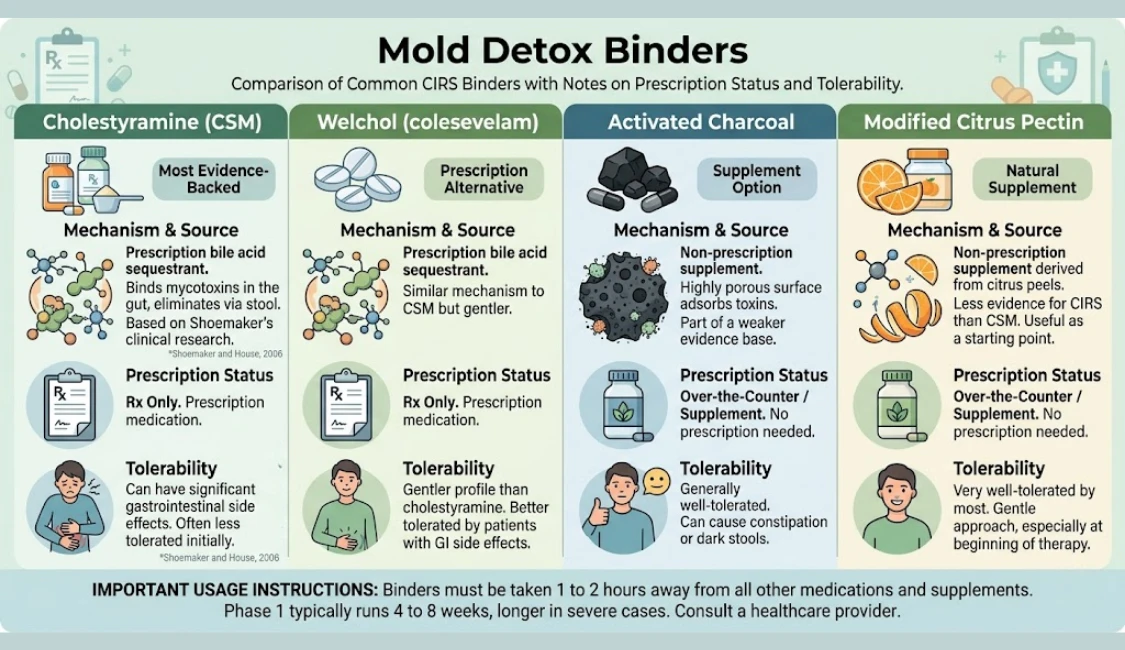
Binders used in clinical practice:
Binders must be taken 1 to 2 hours away from all other medications and supplements. This step typically runs 4 to 8 weeks, longer in severe cases.
This is the step most practitioners miss. It is the reason so many patients plateau.
MARCoNS (Multiple Antibiotic Resistant Coagulase Negative Staphylococcus) is a treatment-resistant staph colonizing the deep nasal sinuses of, in Shoemaker’s clinical data, roughly 80% of CIRS patients. It produces hemolysins that directly suppress alpha-MSH, one of the body’s central inflammatory regulators. As long as MARCoNS is active, MSH cannot normalize, and the downstream cascade continues: sleep dysregulation, immune activation, hormonal disruption. Neither MSH nor MARCoNS appears on standard panels. Neither will show up unless someone specifically orders them.
Testing requires a deep nasal culture at a specialty lab (MicrobiologyDX). Treatment is BEG spray (compounded Bacitracin, EDTA, Gentamicin) twice daily for 30 days, followed by a repeat culture to confirm clearance.
The rule: VIP cannot start until MARCoNS is confirmed cleared. VIP in the presence of active MARCoNS worsens the colonization and derails months of progress.
Once binders have reduced the toxin load and MARCoNS has been cleared, the body often begins recovering regulatory hormone production on its own. When it doesn’t, we support it directly.
MSH (alpha-Melanocyte Stimulating Hormone): The neuropeptide whose suppression drives most downstream CIRS pathology: sleep dysfunction, gut motility problems, pain amplification, cytokine dysregulation. MSH often recovers with binder therapy and MARCoNS clearance. When it doesn’t, VIP is the next step.
VIP (Vasoactive Intestinal Peptide): Shoemaker’s research reports VIP deficiency in approximately 98% of CIRS patients. VIP nasal spray has been used in over 10,000 CIRS patients with documented efficacy in normalizing brain inflammation, restoring grey matter atrophy, and correcting inflammatory transcriptomics refractory to other therapies. (Shoemaker, House, and Ryan, 2013) NeuroQuant MRI research confirmed that CIRS patients show structural brain changes and that VIP can reverse some of that atrophy. (Shoemaker, House, and Ryan, 2014) See our VIP peptide overview for dosing and timing guidance.
Other markers corrected in this step: C4a, TGF-beta 1, VEGF (often low, driving fatigue and air hunger), and ACTH/cortisol if the adrenal axis has been disrupted.
The Shoemaker protocol was designed for CIRS as a standalone condition. For many of the patients I see, it isn’t standalone. Lyme disease, MCAS, and co-infections frequently accompany CIRS, and when they do, they have to be addressed explicitly or treatment stalls.
Lyme and CIRS together: Lyme drives a Th1-dominant inflammatory response on top of CIRS’s biotoxin cascade. Neither resolves when treatment targets only one. Aggressive Lyme antibiotic therapy in a patient with high mycotoxin burden produces Herxheimer reactions an already-compromised immune system handles poorly. Reducing the biotoxin burden first creates a more stable baseline. See Lyme disease and biotoxins for more on how these conditions interact.
MCAS: Mast cell activation is common in this population. The hypersensitive mast cell response makes binder therapy and Lyme treatment harder to tolerate. We stabilize it alongside the CIRS protocol: H1 and H2 antihistamines, quercetin, low-histamine dietary modification.
Limbic system: A subset of patients clears their biotoxin burden but remains sensitized and unwell. Prolonged neuroinflammation can lock the limbic system into a chronic alarm state after the original threat is gone. Structured limbic system retraining such as DNRS or the Gupta Program, combined with vagus nerve work, can break that loop.
Correct sequencing starts with correct diagnosis. The testing panel that confirms CIRS and guides treatment includes:
Standard labs (CBC, CMP, TSH, ANA) are almost always normal in CIRS. Normal labs don’t mean normal health. They mean the wrong tests were ordered.
Timeline depends on how long the exposure lasted and whether Lyme or MCAS co-exists.
Recovery is not linear. Setbacks occur with re-exposure or Herxheimer reactions. The most important variable is starting: every additional month of untreated CIRS adds to the biotoxin load and downstream damage.
Not every clinician familiar with mold illness knows the full Shoemaker sequence, the MARCoNS testing requirement, or the Lyme/MCAS overlap. If you have been told “CIRS isn’t real,” if MARCoNS has never been tested, or if Lyme treatment keeps producing crashes, those are signals to broaden your care team. Our mold illness treatment overview has guidance on what to look for in a provider.
If you are managing Lyme disease alongside CIRS, working with a Lyme disease specialist who understands the biotoxin overlap is the most direct path forward.
The Shoemaker protocol is a sequential framework developed by Dr. Ritchie Shoemaker. It removes biotoxin exposure, uses bile acid sequestrants to clear mycotoxins, addresses MARCoNS nasal colonization, corrects hormone deficiencies (MSH, ACTH, VIP), and restores inflammatory marker balance. A 2024 systematic review confirmed it is the only CIRS treatment with documented clinical efficacy.
Roughly 25% of people carry HLA-DR gene variants that prevent normal mycotoxin clearance. Moving out removes the exposure source but does not clear what is already in the body. Biotoxins continue to circulate, inflammatory markers stay elevated, and hormonal pathways remain disrupted. CIRS requires a sequenced treatment protocol, not just relocation.
Cholestyramine (CSM) is the most evidence-backed option, a prescription bile acid sequestrant that interrupts mycotoxin recirculation. Welchol (colesevelam) is a prescription alternative with a gentler GI profile. Supplement-based options include activated charcoal, modified citrus pectin, and binding clays. All binders must be taken 1 to 2 hours away from other medications.
Timeline depends on how long the exposure lasted and whether Lyme or MCAS co-exists. Patients without concurrent infections often see measurable improvement within 3 to 6 months, substantial recovery by 12 to 18 months. Patients with active Lyme or MCAS typically require 18 to 24 months. Recovery is real but not linear.
Cholestyramine has the strongest evidence base, but patients who cannot tolerate it have options. Welchol is a prescription alternative with a gentler GI profile. Activated charcoal, modified citrus pectin, and bentonite clay may reduce the biotoxin burden, though evidence is weaker. Some form of active binding is required: the body cannot clear recirculating mycotoxins without a sequestrant.
VIP (vasoactive intestinal peptide) is deficient in approximately 98% of CIRS patients. VIP nasal spray normalizes brain inflammation and corrects inflammatory transcriptomics that persist despite earlier treatment. It must only begin after MARCoNS is confirmed cleared. VIP in the presence of active MARCoNS worsens the nasal colonization.
If you have done everything you were told and still don’t feel like yourself, you may need someone who treats the full picture: CIRS, Lyme, MCAS, and the nervous system together. My practice serves patients in CO, WY, NJ, PA, TX, and WI via telehealth.
Book an Initial Consultation – $300
Telehealth. No referral needed. Comprehensive intake before your first visit.
Author: Dr. Diane Mueller, ND, LAc, DAOM
Medical Disclaimer: The information in this article is intended for educational purposes only and does not constitute medical advice, a diagnosis, or a treatment recommendation. CIRS and biotoxin illness are complex medical conditions requiring individualized evaluation by a qualified clinician. Do not begin or discontinue any treatment based solely on the information presented here. If you are experiencing symptoms described in this article, consult a licensed healthcare provider experienced in CIRS and biotoxin illness.