


You’ve been told you’re allergic to everything. Foods that were never a problem now send you spiraling. A scent in the grocery store makes your throat tighten. You’ve been dismissed by doctors who looked at your allergy tests, saw nothing flagged, and suggested anxiety.
Every reaction you are having is real. Every one of them is measurable.
What you are describing is mast cell activation syndrome (MCAS), and the “react to everything” pattern is one of its most consistent presentations. Many of the patients we see have spent years having their symptoms managed while no one asked the more important question: why did the mast cells become hyperreactive in the first place? In our practice, that question is where MCAS treatment begins.
Quick Answer: MCAS treatment works in a stepwise sequence: identify and remove triggers; stabilize mast cells with H1 and H2 antihistamines and mast cell stabilizers like cromolyn sodium or quercetin; support with a low-histamine diet; then identify and treat the underlying driver (Lyme disease, mold/CIRS, or gut dysbiosis in most patients). Treating symptoms without addressing the root driver is why so many patients improve partially but never stabilize fully.

Here is what is actually happening in your body. Mast cells are immune cells that sit in the tissues most exposed to the outside world: your skin, GI tract, lungs, and connective tissue. Their job is early-threat detection. When they sense a pathogen or toxin, they degranulate (release their stored contents), sending out histamine, prostaglandins, and other inflammatory messengers.
In MCAS, that release becomes dysregulated. The cells fire inappropriately and repeatedly, producing symptoms across several systems at once: flushing, hives, GI cramping, a racing heart, brain fog, fatigue. Because this is not a classic allergy, it responds inconsistently to standard allergy treatment. That is precisely why so many people are told their tests look normal while they continue to react to nearly everything.
A 2021 critical review confirms that MCAS diagnosis requires compatible recurrent symptoms, mast cell mediator evidence, and clinical response to anti-mediator therapy. Gülen et al., 2021 For the full diagnostic picture, see our page on what MCAS is and how it develops.
The treatment question is not “how do we quiet the mast cells?” It is “what is keeping them in chronic alarm?”
No medication works as well as it should if the triggers activating your mast cells are still present. This step comes first.
Triggers fall into several categories:
Environmental: Mold, fragrances, cleaning products, smoke, pollens, and temperature extremes. Mold is the most consequential and most often missed. Mycotoxins from water-damaged buildings are potent mast cell activators. If reactions worsened after a move or renovation, evaluate the environment before assuming the immune system is deteriorating on its own. See our page on mycotoxin illness for more.
Food: High-histamine foods (aged cheeses, fermented foods, alcohol, canned fish, leftovers) and histamine liberators (strawberries, citrus, shellfish, certain additives). Triggers are individual: what one patient reacts to reliably, another tolerates without issue.
Physical and emotional stress: Heat, cold, exercise, and emotional stress all drive mast cell degranulation through the autonomic nervous system.
Infections: Active infections, including Lyme disease and co-infections, are significant mast cell activators. Covered in Step 4.
Medications and supplements: NSAIDs, certain antibiotics, opioids, and contrast dye are known triggers. Some patients also react to binders, herbs, or B vitamins, which is relevant when starting treatment.
A symptom-and-trigger journal for the first four to six weeks is often the most useful early tool. Reactions that appear random frequently reveal consistent patterns when tracked.
Once major triggers are reduced, the goal is to lower the mast cell’s reactivity threshold so remaining triggers produce less severe responses.
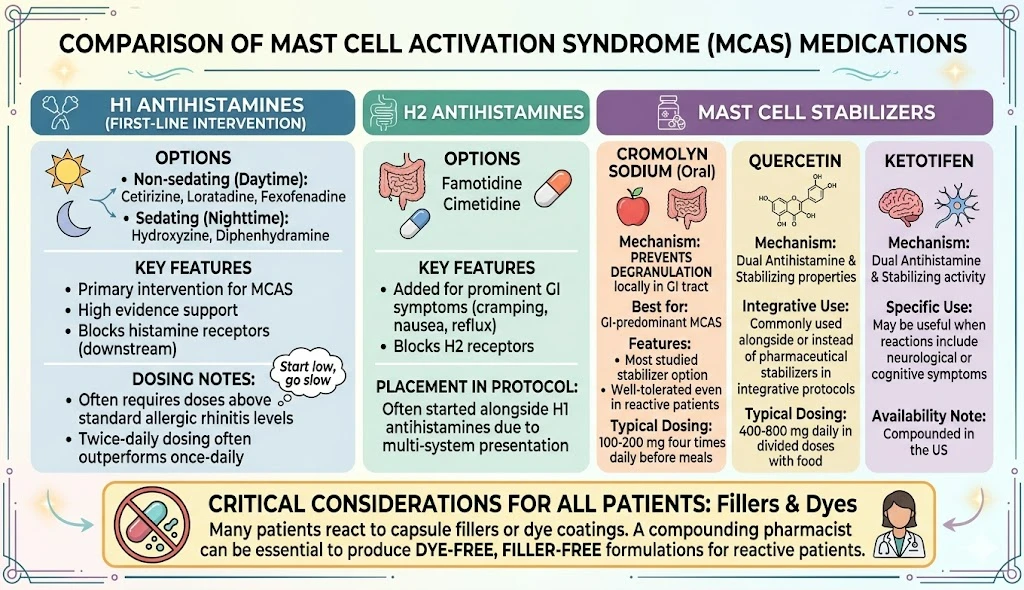
H1 antihistamines are the most evidence-supported first-line intervention for primary MCAS. Nurmatov et al., 2015 Non-sedating options (cetirizine, loratadine, fexofenadine) are used during the day; sedating options (hydroxyzine, diphenhydramine) at night. Many MCAS patients require doses above standard allergic-rhinitis levels, and twice-daily dosing often outperforms once-daily.
Adding an H2 antihistamine (famotidine, cimetidine) is standard when GI symptoms (cramping, nausea, reflux) are prominent. Many clinicians start H1 and H2 together given how common multi-system presentation is.
Stabilizers prevent degranulation rather than blocking histamine downstream.
Cromolyn sodium (oral) is the most studied option for GI-predominant MCAS. It acts locally in the GI tract and is well-tolerated even in reactive patients. Typical dosing: 100-200 mg four times daily before meals.
Quercetin (400-800 mg daily in divided doses with food) has both antihistamine and stabilizing properties and is commonly used alongside or instead of pharmaceutical stabilizers in integrative protocols.
Ketotifen (compounded in the US) has dual antihistamine and stabilizing activity; may be useful when reactions include neurological or cognitive symptoms.
Start low, go slow. Many patients react to capsule fillers or dye coatings; a compounding pharmacist who produces dye-free, filler-free formulations can be essential for the most reactive patients.
Diet reduces total histamine load while treatment takes effect. It is a therapeutic tool for the stabilization phase, not a permanent dietary identity.
Minimize: aged cheeses, fermented foods, alcohol, canned and smoked fish, cured meats, vinegar, and leftover proteins (histamine accumulates as protein sits).
Watch individually: citrus, strawberries, tomatoes, spinach, and avocado are histamine liberators or contain biogenic amines that compete for the same degradation enzyme (DAO). Individual tolerance varies.
Fresh proteins cooked and eaten immediately, well-tolerated vegetables, and non-citrus fruits form the foundation. Systematic reintroduction once reactivity improves is essential: long-term blanket restriction often reflects undertreated illness rather than a permanent dietary ceiling.
For concurrent SIBO or gut dysbiosis, see our page on dietary approaches for gut-related chronic illness.
Mast cells do not become hyperreactive without a reason. In our experience, that reason is almost always an upstream driver: an ongoing infection, a biotoxin burden from mold exposure, gut dysbiosis (an imbalance in the gut bacteria), or some combination of the three. Until that driver is addressed, mast cell stabilization is damage control. It helps, and it does not resolve.
This is the difference between managing MCAS and changing its course. It is also the step most standard workups skip, not because your clinician doubted you, but because this intersection of infection, biotoxins, and immune reactivity sits outside what most conventional training covers.
Lyme disease is one of the most underrecognized MCAS drivers. Research published in Infection and Immunity demonstrated that Borrelia burgdorferi spirochetes directly activate mast cells and stimulate cytokine release. Talkington et al., 1999 A chronic Lyme infection is not merely coexisting with MCAS. It may be the source of it.
The pattern is recognizable: a patient develops Lyme (sometimes without knowing it), then develops expanding reactivity to foods, fragrances, and medications over months or years. Bartonella and other co-infections add their own immune disruption. See our page on Lyme co-infections including Bartonella for evaluation details.
Antihistamines reduce individual reactions but do not address the bacterial driver. Treating Lyme and co-infections is often what moves a patient from “manageable with medication” to genuinely stable.
Mycotoxins from water-damaged buildings are direct mast cell activators. In patients with HLA-DR susceptibility genes (roughly 24% of the population, per Shoemaker’s CIRS clinical research), mycotoxin exposure also triggers Chronic Inflammatory Response Syndrome (CIRS), a self-amplifying inflammatory state that keeps mast cells in a chronic activation loop. Antihistamines cannot override this burden: the CIRS inflammatory state must be addressed. See our page on CIRS symptoms for the diagnostic picture.
The gut is the largest site of mast cell concentration in the body. Research published in Biomolecules documents a bidirectional gut microbiota-mast cell axis: dysbiosis and intestinal permeability increase mast cell activation, while mast cell degranulation further disrupts the barrier and microbiome, a mechanism with direct relevance to MCAS patients with gut involvement. Carnevale et al., 2026 For patients with expanding food intolerances, bloating, or altered bowel habits, gut evaluation is not optional. SIBO, Candida overgrowth, and low-diversity microbiomes all contribute to mast cell hyperreactivity.
The autonomic nervous system directly triggers mast cell degranulation. A body locked in chronic stress (from pain, trauma, or long illness) keeps driving reactivity even when the other steps are in place. For patients who have stabilized on medication and addressed root drivers but remain reactive to emotional or sensory stimuli, vagal nerve work (slow breathing, humming, cold-water exposure) and structured limbic system retraining are the next layer.
For how to recognize this pattern in the context of chronic illness, see our page on nervous system dysregulation symptoms. These approaches complement medical care; they do not replace it.
If your MCAS treatment has stalled, if no one has evaluated you for Lyme disease or mold exposure, or if your reactions keep expanding despite antihistamines, a comprehensive root-cause evaluation may change everything. Our practice serves patients in CO, WY, NJ, PA, TX, and WI via telehealth.
Book an Initial Consultation – $300
Telehealth. No referral needed. Comprehensive intake before your first visit.
The goal is not to eliminate all symptoms immediately. The realistic trajectory:
Phase 1 (weeks 1-8): Identify and reduce reliable triggers. Start H1 and H2 antihistamines and introduce a low-histamine diet. Some patients improve significantly within weeks; those with an active root driver typically see partial improvement only.
Phase 2 (months 2-6): Evaluate for root drivers (Lyme, CIRS, gut dysbiosis). Treating confirmed drivers allows reactivity to continue improving as the upstream source is addressed. Dietary expansion becomes possible.
Phase 3 (months 6-18+): Sustained reduction in reactive episodes. For patients with concurrent Lyme, this phase runs parallel to Lyme treatment; Herxheimer reactions can transiently worsen mast cell reactivity and must be anticipated.
A 2021 paper in Allergy and Asthma Proceedings addresses persistent misconceptions about MCAS that can delay appropriate treatment. Zhang et al., 2021 Patients who achieve the most improvement share one trait: they stayed with the full protocol rather than only the layers that provided quick relief.
Not every clinician is trained to evaluate the intersections of MCAS with Lyme, mold, and gut dysbiosis. Consider working with a specialist if:
Working with a Lyme and mold-literate specialist is often what changes the trajectory from partial management to actual recovery. Dr. Mueller had Lyme disease herself: personal experience and specialized training shape how she approaches patients who have been reactive to everything and dismissed by everyone.
First-line treatment begins with trigger identification and H1 antihistamines for flushing, hives, and itching. H2 antihistamines are added for GI involvement. Mast cell stabilizers like cromolyn sodium or quercetin are typically introduced in the same phase. This symptom-management layer is necessary, but it is not the same as treating why the mast cells became hyperreactive.
MCAS does not have a predictable fixed endpoint, but many patients achieve significant long-term stability. Whether a patient improves substantially depends on whether the underlying driver is identified and treated. Patients with MCAS driven by Lyme, mold/CIRS, or gut dysbiosis often see far more improvement when those root conditions are addressed alongside mast cell stabilization.
The low-histamine approach limits aged cheeses, fermented foods, alcohol, canned fish, vinegar, and leftover proteins. Individual triggers also vary: some patients react to oxalates, gluten, nightshades, or food additives. A short-term elimination diet with supervised reintroduction is more useful than permanent blanket restriction.
Yes. Research confirms that Borrelia burgdorferi spirochetes directly activate mast cells and trigger cytokine release. A chronic Lyme infection can keep the immune system in persistent mast cell activation. Many patients with Lyme-associated MCAS find that antihistamines help somewhat but they do not stabilize until the underlying infection and co-infections are addressed.
Mycotoxins from water-damaged buildings are potent mast cell activators. In genetically susceptible individuals, exposure can tip a borderline immune system into full MCAS reactivity or dramatically worsen existing MCAS. Addressing mold exposure and treating the biotoxin burden is often what allows reactivity to stabilize.
It can, for a specific subset of patients. Mast cells are directly innervated by the autonomic nervous system: a nervous system locked in chronic stress actively drives degranulation. For patients who have stabilized on medication and addressed root drivers but remain reactive to emotional or sensory stimuli, limbic retraining and vagal nerve work can reduce baseline reactivity. These complement medical treatment; they do not replace it.
Medical Disclaimer: The information in this article is intended for educational purposes only and does not constitute medical advice, a diagnosis, or a treatment recommendation. Mast cell activation syndrome is a complex medical condition that requires individualized evaluation by a qualified clinician. Do not begin or discontinue any treatment based solely on the information presented here. If you are experiencing a medical emergency or severe allergic reaction, call 911 or go to your nearest emergency room.