


Quick Answer: Yes, and the mechanism is biological, not psychological. Mycotoxins suppress alpha-MSH (disrupting serotonin and melatonin), trigger neuroinflammation in the limbic system, and push the autonomic nervous system into chronic sympathetic dominance. The result is anxiety, panic, and depression that can closely resemble primary mood and anxiety disorders, yet typically does not respond to SSRIs because the biotoxin driver is never addressed. Patients typically have co-occurring physical symptoms (brain fog, fatigue, unusual sensitivities) that together point toward a mold workup rather than a psychiatric diagnosis.
“I was never an anxious person before this. And no one believes me.” That sentence comes up in my practice more than almost any other. A patient who was calm and functional before a move, renovation, or new building. Then anxiety from nowhere, panic attacks with no trigger, SSRIs that don’t work. Years pass. No one ever checks the building.
If that arc sounds familiar, here is the biology behind it.

When you inhale mycotoxins, research suggests inhaled mycotoxins can penetrate the central nervous system and activate microglia, which release pro-inflammatory cytokines including TNF-alpha, IL-1 beta, and IL-6. Animal studies show that trichothecene mycotoxins produce central neuroinflammation by upregulating these cytokines in brain tissue (Bonnet et al., 2012). Studies in mice found that Satratoxin G from Stachybotrys chartarum caused direct damage to olfactory neurons and marked cytokine expression in the olfactory bulb, which sits immediately adjacent to the amygdala, a finding consistent with the neuroinflammatory pathway proposed in human CIRS (Islam et al., 2006). A 2009 clinical review documents that mold and mycotoxin exposure produces neuropsychiatric features including anxiety and mood changes (Empting, 2009).
When the amygdala is inflamed, it fires more easily, interprets more stimuli as threatening, and does not calm down normally. The result is a nervous system locked in hypervigilance: excessive worry, physical arousal, sleep disruption, and a body that cannot stand down from a danger signal it cannot identify. The mood component is not separate from the physical symptoms: both are produced by the same neuroinflammatory process. For the full neurological picture, see our guide to neurological symptoms of mold exposure.
In Chronic Inflammatory Response Syndrome (CIRS), mycotoxin exposure suppresses alpha-MSH, a hypothalamic neuropeptide that regulates serotonin synthesis, melatonin cycling, and inflammatory tone. When MSH drops, serotonin decreases and melatonin cycling destabilizes, producing anxiety, panic, and depression that can mirror primary psychiatric disorders symptom for symptom. SSRIs often fail because they work downstream on reuptake while the production pathway is disrupted upstream. Shoemaker and House documented MSH suppression and the downstream hormonal burden of CIRS in water-damaged building patients. (Shoemaker and House, 2006)
Not everyone exposed to mold develops anxiety at this severity. Shoemaker’s clinical research estimates roughly 25% of the population carries HLA-DR gene variants that impair mycotoxin clearance. In these individuals, toxins recirculate through enterohepatic recirculation and are repeatedly reabsorbed. Neurological and mood consequences are more severe, more persistent, and do not resolve after leaving the moldy building. The anxiety can continue for years while conventional medicine searches for a psychiatric explanation. Full CIRS presentation: CIRS symptoms.
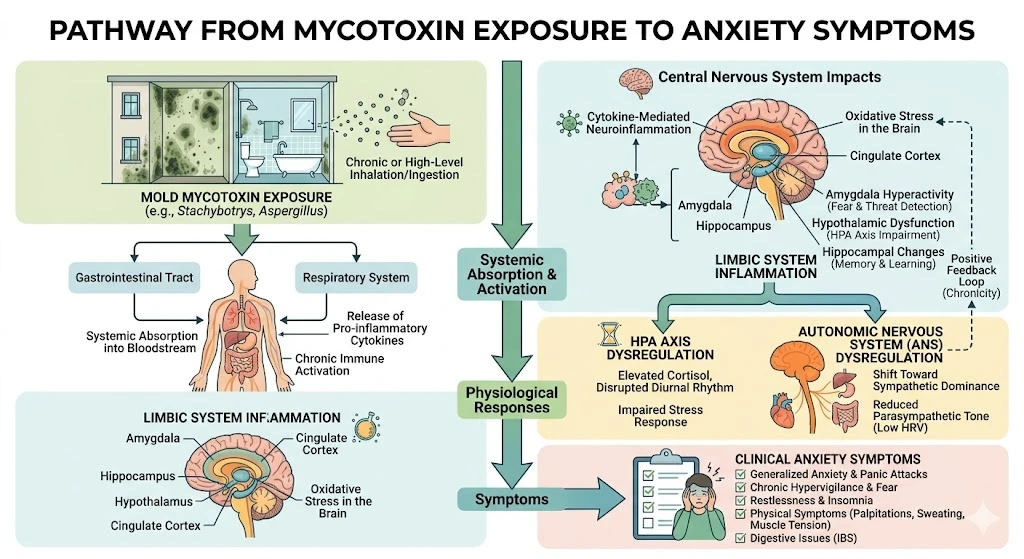
Beyond the chemical mechanism, mold sets off a structural loop that compounds anxiety independently of ongoing exposure. The limbic system settles into persistent hyperarousal; the hypothalamus loses its ability to regulate sympathetic (fight-or-flight) vs. parasympathetic balance. The result: chronically “on,” scanning for threat, unable to rest, anxious for no reason, can’t turn off at night, wired and exhausted simultaneously. This nervous system component requires its own treatment, separate from biotoxin clearance. See our guide on nervous system dysregulation symptoms.
No single feature is definitive. But a pattern of features together makes a strong case for mold as a driver.
The onset story matters. Anxiety that began or worsened after a move, renovation, flood, or new building, and worsens each time you return to that space, is pointing somewhere physical. Primary anxiety disorders tend to emerge gradually in the context of psychological stressors, not environmental ones.
Location dependence is the most telling sign. Anxiety that reliably improves when you leave home and worsens on return, with a mood crash within 24-48 hours, points to the building, not your psychology.
Physical symptoms that don’t fit the psychiatric diagnosis. Mold-toxic patients almost never present with anxiety alone. Brain fog, air hunger, light sensitivity, ice-pick pains, and fatigue unresolved by sleep are not explained by primary anxiety disorder. When these co-occur, a mold illness symptoms workup belongs in the differential.
Non-response to standard psychiatric medication. Multiple SSRI, SNRI, or benzodiazepine failures without lasting relief is a clinical signal that the biotoxin root cause has not been addressed.
Mast Cell Activation Syndrome (MCAS) frequently co-occurs with mold illness and produces anxiety-like symptoms through histamine release, including panic attacks and adrenaline surges. If anxiety flares unpredictably with reactions to foods, perfumes, or medications rather than psychological stress, MCAS symptoms should be part of your evaluation.
Most psychiatrists are not trained to look for mold as an anxiety driver. The pattern is consistent: anxiety develops after an environmental change that goes unrecognized; routine labs return normal; a psychiatric diagnosis is made; medication produces partial or absent response; years pass while the biology progresses. The anxiety, brain fog, and mood instability are expressions of the same inflammatory process. If cognitive symptoms accompany the mood changes, our article on whether mold can cause memory loss covers the overlapping mechanisms.
Standard workups will not catch mold-driven anxiety. A normal TSH, CBC, and metabolic panel do not rule out CIRS. The right tests are specialized and rarely ordered in conventional settings. Here is the sequence I use with patients presenting with possible mold-related mood symptoms.
Visual Contrast Sensitivity (VCS) Test: Free at survivingmold.com. Detects biotoxin-related neurological impairment through the visual pathway. A failed VCS in a patient with unexplained anxiety is a significant indicator of CIRS.
Urine Mycotoxin Panel: Mosaic Diagnostics (formerly Great Plains) or Vibrant America’s Real-Time Labs. Tests for ochratoxin A, trichothecenes, gliotoxin, and aflatoxins. Some patients require a brief provocation protocol (sauna or glutathione) for better detection.
These markers are the core of a proper CIRS diagnostic workup:
Patients with CIRS show statistically significant structural brain changes on volumetric MRI vs. healthy controls, underscoring why early diagnosis matters. (Shoemaker et al., 2014)
HLA-DR Genotyping (LabCorp or Quest) identifies whether you carry susceptibility haplotypes. Combined with a positive mycotoxin panel and abnormal CIRS markers, it confirms the treatment framework. A Lyme disease specialist trained in CIRS will know how to interpret and act on this panel.
MARCoNS Nasal Culture (MicrobiologyDX) tests for multi-antibiotic resistant staph in the deep nasal sinuses (present in approximately 80% of CIRS patients per Shoemaker’s clinical data). MARCoNS suppresses MSH independently of mycotoxin load, worsening mood through a self-perpetuating cycle.
Mold-driven anxiety does not respond to psychiatric treatment alone. The sequence matters.
Nothing resolves while the exposure continues. ERMI environmental testing identifies the source. For genetically susceptible patients, even low-level re-exposure restarts the cascade.
Bile acid sequestrants interrupt enterohepatic recirculation of mycotoxins. The most studied options: cholestyramine (CSM), Welchol (colesevelam, for CSM-intolerant patients), and supplement-based binders (GI Detox, activated charcoal). Typical duration 4-8 weeks with follow-up testing to confirm reduction. See binders for mold detox for sequencing detail.
MARCoNS colonization suppresses MSH independently of the mycotoxin load. Standard treatment is BEG nasal spray (Bacitracin, EDTA, Gentamicin), twice daily for 30 days, with repeat culture before advancing. Once MARCoNS is cleared and biotoxin burden is down, MSH often normalizes. When it remains suppressed, VIP (vasoactive intestinal polypeptide) nasal spray restores the serotonin and melatonin pathways. It is prescription-only and must not be used while MARCoNS is active. Full treatment detail: mold illness natural treatment.
After the biotoxin burden is down and confirmed on follow-up labs, some patients remain in limbic hyperarousal. The inflammatory trigger is gone, but the nervous system has not adjusted. Limbic system retraining addresses this physiological loop. Structured brain retraining programs (DNRS, Gupta Program) combined with vagus nerve work (slow breathing, cold exposure) can shift the autonomic baseline from sympathetic to parasympathetic dominance. This is not a substitute for clearing the mold. It is the final phase for patients who are “technically recovered” on labs but still feel anxious. Skipping it is the most common reason that recovery stalls.
Yes. Mycotoxins trigger limbic neuroinflammation, suppress alpha-MSH (disrupting serotonin and melatonin), and drive sympathetic dominance. Together these produce anxiety and panic attacks that can be difficult to distinguish from primary panic disorder, yet typically do not respond to psychiatric medication because the biotoxin driver is never addressed.
Key indicators: anxiety that began or worsened after an environmental change; anxiety that improves when you leave home and worsens on return; unexplained physical co-symptoms (brain fog, fatigue, air hunger, sensitivities); and non-response to multiple psychiatric medications. Start with the VCS test, urine mycotoxin panel, and CIRS markers (C4a, TGF-beta 1, MSH).
Yes. MSH suppression disrupts serotonin production and melatonin cycling, the same pathways antidepressants target, producing symptoms that can closely resemble primary depression. Patients typically do not respond to SSRIs because the biotoxin root cause is never addressed. Depression paired with brain fog, fatigue, and unusual sensitivities warrants a mold workup in the differential.
Location-dependent anxiety is a strong clinical signal for mold exposure. The limbic system sits adjacent to the olfactory bulb, where mold damage registers first, producing a near-immediate alarm response in contaminated environments, sometimes before the person consciously notices anything unusual. If anxiety reliably improves when you leave a building and worsens on return, the building deserves investigation.
Alpha-MSH regulates serotonin availability and melatonin cycling. Mycotoxin exposure suppresses MSH below normal, decreasing serotonin and destabilizing sleep. Mold-toxic patients often do have low serotonin, but SSRIs alone typically do not resolve the deficiency because it is downstream of MSH suppression, not a primary psychiatric condition.
In the roughly 25% of people with HLA-DR susceptibility variants, mold-driven anxiety can persist long after leaving the moldy environment because mycotoxins recirculate rather than clear, MSH suppression continues, and the limbic system stays in chronic alarm. Leaving the building is necessary but not sufficient. Active biotoxin clearance, hormonal pathway restoration, and limbic retraining are all required.
If your anxiety has not responded to standard treatment, if it started after entering a new environment, or if it comes packaged with brain fog, fatigue, and symptoms no one can explain, a comprehensive mold and CIRS workup may be the evaluation you have never had. I work with patients across CO, WY, NJ, PA, TX, and WI via telehealth.
Book an Initial Consultation – $300
Telehealth. No referral needed. Comprehensive intake before your first visit.
Author: Dr. Diane Mueller, ND, LAc, DAOM
Medical Disclaimer: The information in this article is intended for educational purposes only and does not constitute medical advice, a diagnosis, or a treatment recommendation. Anxiety and mood symptoms have many causes. Mold-related illness and CIRS require individualized evaluation by a qualified clinician. Do not begin or discontinue any treatment, including psychiatric medication, based solely on the information presented here. If you are experiencing a mental health crisis, contact the 988 Suicide and Crisis Lifeline by calling or texting 988.